|
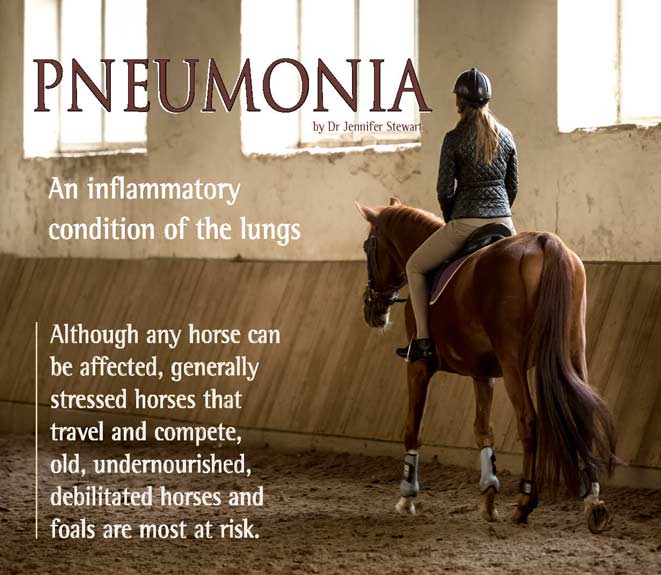
Pneumonia is usually classified by the cause: bacterial, viral, fungal, chlamydial, parasitic, aspiration, allergic or toxic/chemical – but in many cases no cause can be identified. In Arabian horses, combined immunodeficiency (CID) should also be considered. 
To enable your veterinarian to prescribe the most appropriate therapy, diagnosis of pneumonia and determining the exact cause requires a thorough work-up. Diagnostic investigation may include blood tests, ultrasound to visually assess the extent of damage on the lung surface, xrays and a tracheal wash to collect a sterile fluid sample from the lungs that can be submitted for culture and sensitivity to antibiotics.
BACTERIAL
Streptococcus equi ssp. zooepidemicus, is related to the strangles bacteria and is a normal resident of the upper respiratory tract of healthy horses. It is the most commonly identified organism in 72% of cases of pneumonia and its presence in the lung tissue is associated with severe and extensive damage. And it can also infect humans – i.e. it has zoonotic potential. S. zooepidemicus is a risk for people working with sick horses and can cause meningitis, endocarditis, arthritis, abscesses, and sepsis (blood poisoning). So the importance of early detection, biosecurity protocols to prevent spreading of this dangerous germ, and proper management of equine pneumonia cannot be stressed enough.
AIR QUALITY
To reduce the risk of respiratory irritation, infections and pneumonia, air quality is obviously important in stables and arenas. Airborne dust in the stable environment is composed of plant fragments, mites, bacteria and mould spores, yeasts, and endotoxins, with the level and composition being influenced by the choice of bedding, forage and activities, such as mucking out and sweeping. Mucking out and cleaning the stable corridors should be done when the horses are not in the stables.
Bedding material and forage with low contents of airborne particulate matter (APM) (straw pellets, wood shavings, haylage, and silage) are especially recommended for horses suffering from chronic and allergic equine respiratory disorders. Steaming whole bales of hay can reduce APM by up to 89%. APM mould concentration in the air of a riding arena varies with type and moisture content of the footing material, activity in the riding arena, maintenance condition of the arena, number of horses being trained simultaneously and gait of the horse. Rubber flooring, foam flooring, wood shaving-sand mixes and pure sands generate the least amount of APM. There is little evidence that negative air-ionizers reduce dust, endotoxin (fragments of bacterial cell walls) or fungal spores.
VIRAL
Viral pneumonias are less common than bacterial, but the usual culprits are herpes viruses. Carrier states exist where infected horses show no signs, don’t become sick but do spread the virus. The risk of exposure to these agents is highest in young horses that attend sales and competitive events. The stress of travelling and co-mingling can increase viral shedding and in one study, shedding was found in almost 4% of horses. Equine influenza is a constant cause of outbreaks overseas – fortunately we don’t have to deal with that in Australia – but we do have to include Hendra virus infection in the differential diagnosis of any unvaccinated horse with respiratory symptoms.
|
. |
The primary function of the respiratory system, particularly during exercise, is to transfer oxygen from the air that the horse breathes to the red blood cells. It will then be transported throughout the horse’s body.
In addition, carbon dioxide is eliminated from the body via the lungs.
If this system is compromised in any way it will severely affect the athletic ability of a horse and may even be life-threatening.
The lower airway
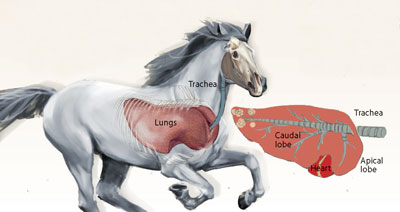
This consists of the lungs and bronchi. The horse lung is divided into the cranial and caudal lobes by the cardiac notch on either side. In addition to these lobes, in the right lung, the accessory lobe is present.
The lungs have protective mechanisms that help
prevent infection.
The air we breathe is not sterile and contains many contaminants such as dirt, dust, pollen and chemicals, as well as bacteria, viruses and fungi.
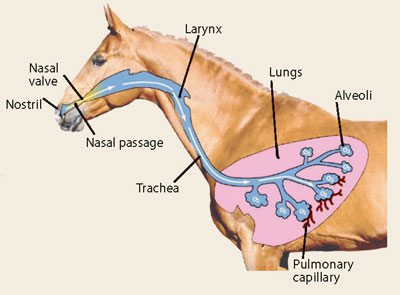
Protection from these contaminants actually starts in the upper airway with filtering, humidifying, and warming of the inspired air.
The Upper Airway
The upper respiratory system, trachea, and bronchi are lined with tissue that is always covered with sticky mucus that traps contaminants. The tissue lining the trachea and bronchi has cells with extremely small hair-like fibers sticking out into the airway called cilia. The cilia increase the surface area of the filtering surface and play an active role in airway protection. The debris that is collected on the surface of the airways is transported away from the lungs by these cilia. The small cilia fibres move in a coordinated rhythm to move the thin layer of mucus that floats on top of the cilia, and the debris that is stuck to it, out of the lungs and up the trachea where the horse will swallow it |
|
| |
|
|
Cases of pneumonia are strongly associated with restraint during transportation (especially cross-tying), when horses are unable to lower their heads. The pooling, puddling and back-flow of normal respiratory secretions down into the lungs instead of out through the nose and mouth, allows bacteria that normally live in the upper respiratory tract to colonise the lungs – resulting in ‘shipping fever’.
Worsening the challenge is that air currents and low humidity reduce the thickness of the respiratory mucus and prevent effective clearance.

Depending on the terrain, exercise can lead to inhalation of sand, grass, water and dirt, further predisposing the lower respiratory tract to contamination and pleuropneumonia. High-intensity exercise can result in a 100-fold increase in bacterial counts in tracheal aspirates.
The yardstick for shipping fever is a rectal temperature of >38.6°C, coughing, nasal discharge and lethargy during transport or soon after. |
|
Take temperatures twice daily, know your horse’s normal temperature and follow the daily temperatures after returning home from a trip. No amount of dollar or expertise can save the sickest of these horses, so those are the ones we really worry about.
Whether a horse gets exposed to a pathogen or inadvertently aspirates food into the trachea while traveling, the result can be a deep bacterial infection. If this progresses to pleuropneumonia – where the lungs and the surfaces of the thorax basically become a giant, inflamed and toxic abcess with pockets of pus and fluid - it becomes increasingly difficult to control. Drainage of pleural effusion results in removal of exudate and debris and allows reexpansion of the lungs, but it is difficult and expensive, requiring thoracic drains and flushing. The prognosis for survival and return to normal athletic function depends on the severity and duration of clinical signs prior to therapy.
When travelling your horse, increasing the rest time and cleaning the interior of the vehicle during rest stops reduces transportation stress and respiratory insults. Being exposed to ammonia while traveling can have devastating effects on the respiratory system.
Ammonia irritates the lining of the airways and horses create high volumes of ammonia (secreted in both urine and manure). Urine can soak into the flooring and rubber mats, providing a constant source of ammonia. Control begins with proper ventilation. Choose a float with ample vents and windows, and refer to the manufacturer’s literature to determine which vents and windows are safe to leave open while travelling. |
Aspiration
Aspiration pneumonia can follow an episode of choke. Signs that indicate that your horse may have an oesophageal obstruction (choke) include enthusiastic feeding then sudden stopping, progressing to discomfort, extension of the head and neck, saliva and feed particles coming out the nostrils. Some of the liquid inevitably goes down the trachea into the lungs. Nearly every choke will have this happen and the risk of aspiration is greater the longer a horse is obstructed. A wait-and-watch approach to see if pneumonia develops is not advisable. It should be treated promptly and rectal temperature monitored to avoid the potential complication of aspiration pneumonia.
Toxic lung injury
This has been recognised in horses after consumption of pyrrolizidine alkaloids, crofton weed, crotolaria, perilla mint, English yew trees, hemlock, brooms, Prunus species, green and night cestrum, mistflower, avocado, red maple and other ornamental plants. And, some agricultural herbicides such as paraquat can induce fatal lung diseases.
GRANULOMATOUS INTERSTITIAL
Granulomatous interstitial pneumonias encompass a wide variety of severe acute and chronic respiratory diseases. They have various causes, including bacteria, viruses and silicate inhalation (silicate pneumoconiosis) caused by inhalation of dust containing crystalline silica.
FUNGAL
Fungal pneumonia usually occurs when the horse’s respiratory system is weakened and the horse inhales fungal spores from mouldy, poor quality hay or other sources.
BUSHFIRE AND SMOKE INHALATION
And of course bushfires and smoke inhalation can cause serious health problems for horses, as it can in people. Smoke particulates, which are a mixture of solid particles and liquid droplets in the air, can irritate horses’ eyes and respiratory tracts and hamper their breathing. Reducing exercise and monitoring for increased respiratory rate or cough should be at the top of our lists when wildfires are near. Ensuring free access to fresh water is also important to keep airways moist and help them clear inhaled particulates.
WORMS
Less frequent causes of pneumonia and respiratory inflammation are worms. Two parasites migrate through the lungs during their life cycle. Roundworm is one of the most common internal parasites of young horses and after being ingested it migrates from the intestine to the liver and then to the lung, where it is coughed up and swallowed to become an adult in the intestine. Foals ingesting large numbers of round worm larvae develop a cough and nasal discharge similar to other respiratory diseases. And the damage from this parasite predisposes young horses to other respiratory diseases. The other offender is equine lungworm which can cause chronic coughing in affected horses – but its main host is donkeys and in most cases, horses acquire lungworm only when pastured with donkeys and when parasite control is not ideal.
Diagnosing parasitic pneumonia is difficult because of the necessity of identifying larvae in the trachea.
CRYPTOCOCCUS
Cryptococcus is a rarely-reported cause of foal pneumonia. It can also cause disease of the lips, nasal passages, sinuses, lungs, liver, colon and brain. In pregnant mares it can cause placentitis and abortion – and can affect future pregnancies. The foal is likely infected via the blood during gestation. A silent focus of infection elsewhere in the mare’s body is the source and abortion or the birth of an infected foal is the result. Another route of mare infection is from environmental contamination during mating or birth. Correct treatment is usually successful.
If you notice any respiratory signs contact your veterinarian without delay. For prevention, minimise stress during travel, be aware of pre-existing conditions that increase risk (Cushing’s disease, Equine Metabolic Syndrome and Inflammatory Airway Disease), stay current with vaccinations and talk to your vet about local conditions. Early intervention and veterinary treatment is key to a successful outcome for most cases of pneumonia – and avoid cough suppressants.
 |
|
with compromised pulmonary function, heat-stress and sun-stroke worsens lung disease, so ensure they have access to shade. High ammonia levels in bedding cause foal lung inflammation and fungicide treatment of wood shavings with pentachlorophenol should be avoided.
Viral pneumonia is usually caused by equine herpes virus 2, which is common in the general horse population.
Fortunately, a vaccination program during the mare’s pregnancy will prevent most cases of viral foal pneumonia, so seek advice from your veterinarian as to how often vaccines need to be administered.
Pneumocystis carinii pneumonia. In Arabian foals with CID, this pneumonia can quickly develop secondary to immunodeficiency.
Bacterial pneumonia sometimes follows viral infections or stressful events that lower the natural lung defence mechanisms. Bacteria are carried into damaged airways or dust may be inhaled from feed, bedding, or working surfaces. In young foals, the most common bacterial causes are
S zooepidemicus with Rhodococcus equi causing an especially severe illness that is associated with contagious outbreaks.
RATTLES caused by a bacteria called Rhodococcus equi is a troublesome and widespread problem - and equine herpesvirus type 2 (EHV-2) is a predisposing factor.
R equi lives in soil and causes pneumonia in 1 to 4 month old foals – and occasionally inflammation of the eyes and joints, bone infection, diarrhoea and abdominal abscesses. It’s found everywhere in the world (except Antarctica) and disease outbreaks vary from year-to-year.
High stocking rates, dry conditions and low grass height are associated with increased risk – all real dangers during drought conditions. Foals inhale or eat the bacteria which then travel via the bloodstream to the lungs. The disease progresses very slowly as large abscesses begin to grow throughout the lungs and eventually the foal shows signs of pneumonia: fever, cough, depression – by which time it can be life-threatening. The antibiotics that treat R equi can cause diarrhoea and over-heating – so caution and careful monitoring are needed - especially in summer. Until a vaccine is available, prevention of rattles is based on early detection by regular ultrasound screening in foals from 30-to-90 days of age.
|
Failure to receive colostrum, overcrowding, cold and damp quarters, environmental irritants, inadequate vaccination and deworming, recent viral respiratory illness, fractured ribs (which occur in 20-65% of foals during birth) and/or any physical condition that weakens the foal may diminish the effectiveness of respiratory tract defence mechanisms. Clinical signs of fractures include increased breathing rate, nostril flare, chest wall swelling and an unwillingness to move or lie down. Ultrasound is much more sensitive than xrays and may be required to identify these injuries.
The majority of foals with pneumonia have bacterial involvement early in the disease. Acute respiratory distress syndrome (ARDS) is a life-threatening condition which can occur secondary to pneumonia, aspiration or blood poisoning. It is likely that a number of different insults lead to ARDS and sudden death in 1-7 month old foals.
In premature or dysmature foals, be on the lookout for signs of respiratory distress – due to incomplete development of the pulmonary structure. In all foals |
| |
|
|
DISCLAIMER
All content provided in this editorial is for general use and information only and does not constitute advice or a veterinary opinion. It is not intended as specific medical advice or opinion and should not be relied on in place of consultation with your equine veterinarian.

OTHER TOPICS available online by Dr Jennifer Stewart
Vol 41- 3
POLTICE IT
Vol 41 - 2
LYME DISEASE IN AUSTRALIA
Vol 41 - 1
I CAN HEAR SAND
Vol 40 - 6
LAMENESS
Vol 40 - 4
STRESS - how do we know if our horse is stressed?
Vol 30 - 1
STIFLE LOCK
with the Equine Veterinarians Australia (EVA)
Vol 27 - 4
ROSS RIVER VIRUS
Vol 36 - 6
BIOSECURITY
Vol 31 - 5
BIG HEAD
Vol 35-6
WHAT CONTROLS APPETITE IN HORSES?
Vol 35 - 4
BEHAVIOUR OR PMS
|